The Kingdom vs. COVID-19
How Saudi Arabia acted swiftly and helped to coordinate a global response to fight the coronavirus, preventing a far worse crisis at home and around the world

'This is the story of Saudi Arabia’s hard-won victory over an unseen killer — a killer vanquished in a war fought not only for the Kingdom but for all people everywhere.'


When the first case of COVID-19 struck Saudi Arabia on March 2, 2020, nobody could have imagined the scale or terrible cost of the battle that lay ahead.
By Monday June 13, 2022, when the Interior Ministry finally announced the lifting of the bulk of precautionary and preventive measures that had been put in place to combat the pandemic, Saudi Arabia had been at war with the SARS-CoV-2 virus for a total of two years, three months and 11 days.
For millions in the Kingdom under lockdown, important life moments were lost forever — birthdays, weddings, anniversaries, even funerals, sacrificed for the greater good, the overriding necessity to protect the nation as a whole.
All understood, however, that all these sacrifices paled into insignificance alongside the suffering of the more than 9,000 people in Saudi Arabia whose lives were claimed by the pandemic, and the agonies endured by their families.
But it could all have been so much worse.
Even as it became clear that the new coronavirus disease that emerged in the final days of 2019 could not be contained in China, many countries were slow to take seriously the threat that the outbreak posed to the lives of their citizens and the health of their economies.
Among those that did act quickly was Saudi Arabia, a nation keenly aware of the consequences — not only for itself and the region but also for the entire planet — if it failed to tackle the pandemic effectively.
The Kingdom had not forgotten the harsh lessons it learned following the eruption within its borders in 2012 of Middle East respiratory syndrome (MERS), an experience that revolutionized Saudi Arabia’s understanding of public-health priorities during a large-scale outbreak of a communicable disease.


It also emerged with the vital understanding that when humankind is faced with a global health crisis, each nation has a responsibility to act in the best interests not only of its own citizens but also of the whole world.
With the outbreak of COVID-19, this responsibility was felt particularly intensely in Saudi Arabia, by far the biggest Arab state in the Gulf and, as custodian of Islam’s holiest sites, responsible every year for the well-being of millions of pilgrims from around the world.
As bad as the global impact of the pandemic has been, how much worse might it have been had Saudi Arabia allowed Hajj to go ahead as normal, risking the possibility of untold numbers of pilgrims returning infected to dozens of countries worldwide?
These were the realities that underpinned Saudi Arabia’s swift response to COVID-19, and which drove its efforts throughout its presidency of the G20 in 2020 to bring the world together to fight the virus in a coordinated way.
This is the story of Saudi Arabia’s hard-won victory over an unseen killer — a deadly foe vanquished in a war fought not only for the Kingdom but for all people everywhere.
How MERS helped the Kingdom prepare for COVID-19


On June 13, 2012, a 60-year-old Saudi citizen with no previous health problems was admitted to a hospital in Jeddah suffering from a fever, cough and shortness of breath. Within 11 days, and despite intensive care, he was dead, killed by the progressive failure of his lungs and kidneys.
MERS-CoV, the sixth coronavirus known to infect humans, had made its deadly debut.
Named MERS in May 2015, this would be the last infectious disease identified by place or region. That same year, the World Health Organization adopted a new protocol for naming human diseases, designed to “avoid causing offense” to any cultural, national or ethnic groups.

Keiji Fukuda, assistant director-general for the WHO, during a press conference on MERS in 2014. Ninety percent of all MERS cases were in Saudi Arabia. (AFP)
MERS, its predecessor severe acute respiratory syndrome (SARS) in 2002-2003 and now COVID-19, are zoonoses — infectious diseases that have jumped from animals to humans. MERS is thought to have originated in camels.
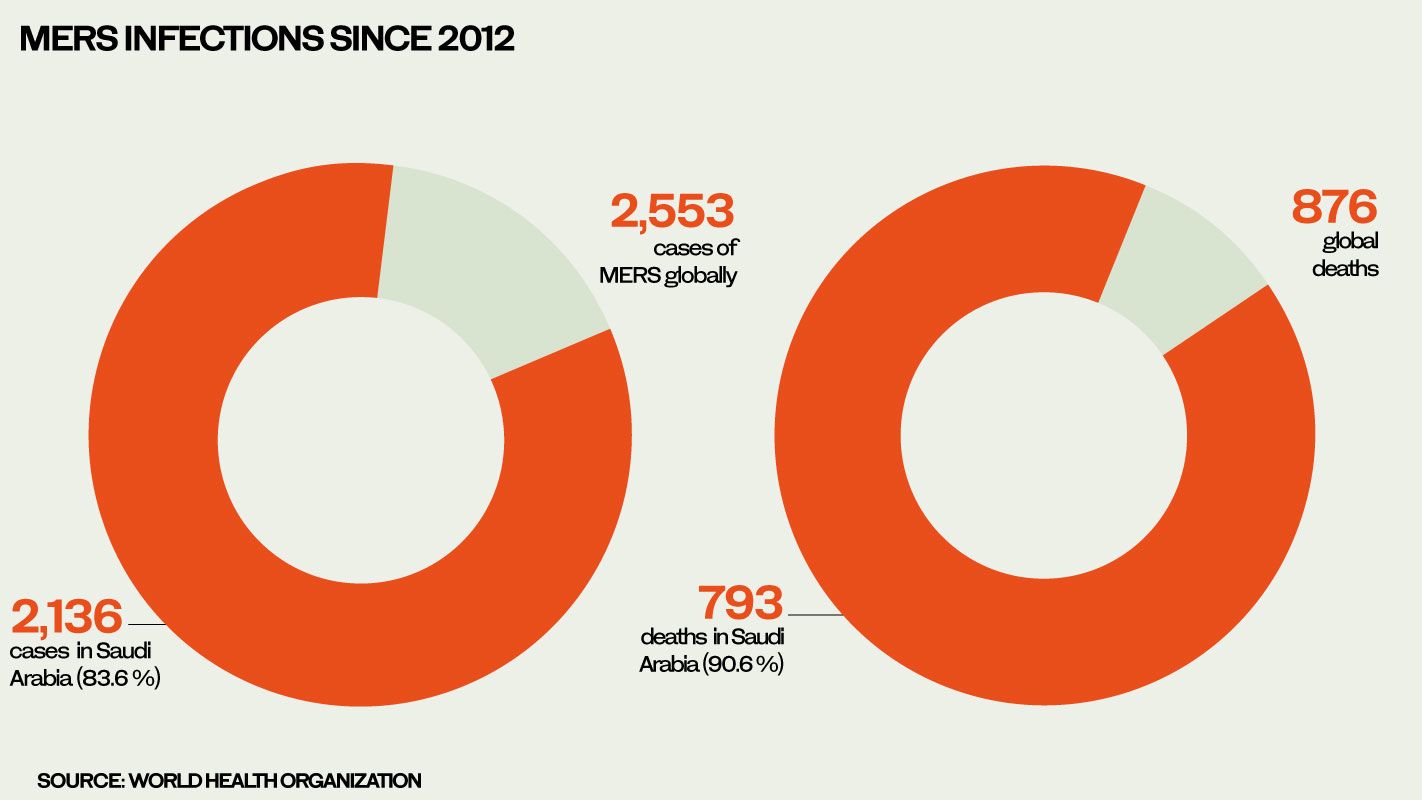
Since 2012, there have been more than 2,500 cases of MERS in 27 countries, claiming the lives of 876 people, but 90 percent of all cases have been in Saudi Arabia.
With a mortality rate of about 35 percent, MERS-CoV kills a far higher proportion of people it infects than SARS-CoV-2, the virus that causes COVID-19. Ironically, it is this lethality that has prevented MERS from becoming as globally devastating as COVID-19; only a live host can continue to spread the disease.
But the virus that causes MERS remains a threat. The most recent serious outbreak in Saudi Arabia occurred between December 2019 and the end of January 2020. Nineteen cases were recorded among residents from six regions, and eight of the patients, seven of them men, died.
The impact of MERS on those families affected by it has been as equally horrific as that of COVID-19. But there is no doubt that the severe shock to the Saudi public health system brought with it lessons that have proved invaluable in the battle against COVID-19.
“Each epidemic, each challenge for the system, serves as a lesson for the leadership of the health sectors in Saudi Arabia,” said Dr. Riyad Qainan Al-Ghamdi, deputy CEO of the Saudi Center for Disease Prevention and Control.
Al-Ghamdi said MERS had given the Kingdom “a very good chance to put in place a very good communication plan within the health care system and between other governmental stakeholders.”
Policies and procedures that were established in response to MERS “were very helpful in accelerating a lot of decisions for this time, and a lot of experiences in policies and procedures and guidelines translated immediately to the response of the current challenge,” he added.
Similarly, Al-Ghamdi said, battling COVID-19 has put Saudi Arabia in a very good place for any future epidemics or pandemics.
Each epidemic, each challenge for the system, serves as a lesson for the leadership of the health sectors in Saudi Arabia.
Dr. Riyad Qainan Al-Ghamdi, deputy chief executive officer of the Saudi Center for Disease Prevention and Control, explains how MERS helped the Kingdom to prepare for COVID-19.
Dr. Riyad Qainan Al-Ghamdi, deputy chief executive officer of the Saudi Center for Disease Prevention and Control, explains how MERS helped the Kingdom to prepare for COVID-19.
Just how dramatically the Kingdom’s health care system was transformed by MERS was summed up in the paper “Preparedness and Response to COVID-19 in Saudi Arabia: Building on MERS Experience,” published in the Journal of Infection and Public Health in June 2020.
The authors, from several Saudi medical institutions, concluded that the emergence of MERS “put Saudi Arabia on a high sense of alert and readiness to take whatever measures (necessary) to curb the spread of COVID-19.”
Since 2012, there have been more than 2,500 cases of MERS in 27 countries.
For example, after the discovery of MERS, the Ministry of Health established a command and control center, and the Saudi Center for Disease Prevention and Control, which have been on the front line of the Kingdom’s response to the current virus.
The ministry also founded the National Health Laboratory to provide advanced diagnostic services for the detection and control of infectious diseases, while “the biosafety in diagnostic laboratories and the application of strict infection prevention and control systems in all hospitals across the country improved substantially.”
More than 25 regional hospitals were designated for the isolation and treatment of MERS patients, and subsequently these hospitals were well prepared to handle those infected with COVID-19.

A nurse walks toward the King Fahad Hospital in Hofuf, east of Riyadh, in 2013. MERS outbreaks were most concentrated in the east of Saudi Arabia. (AFP)
Furthermore, the authors wrote, Saudi Arabia’s medical and scientific research community “demonstrated marvelous efforts in the understanding and control of MERS-CoV in the past few years, as evidenced by more than 480 publications to date, covering both translational and clinical research.”

Keiji Fukuda, assistant director-general for the WHO, during a press conference on MERS in 2014. Ninety percent of all MERS cases were in Saudi Arabia. (AFP)
Keiji Fukuda, assistant director-general for the WHO, during a press conference on MERS in 2014. Ninety percent of all MERS cases were in Saudi Arabia. (AFP)

Since 2012, there have been more than 2,500 cases of MERS in 27 countries.
Since 2012, there have been more than 2,500 cases of MERS in 27 countries.

A nurse walks toward the King Fahad Hospital in Hofuf, east of Riyadh, in 2013. MERS outbreaks were most concentrated in the east of Saudi Arabia. (AFP)
A nurse walks toward the King Fahad Hospital in Hofuf, east of Riyadh, in 2013. MERS outbreaks were most concentrated in the east of Saudi Arabia. (AFP)
How COVID-19 spread in Saudi Arabia


The first case of COVID-19 in Saudi Arabia was announced on Twitter by the Ministry of Health on March 2, 2020. The Saudi patient, who had traveled from Iran via Bahrain over the King Fahd Causeway, was immediately quarantined, and the ministry dispatched infection-control teams to trace and test anyone with whom he had been in contact.
As Arab News noted at the time, until that moment “the Kingdom had been free of the virus for more than three months as it spread from China to 66 countries.”

On March 3, 2000, Arab News reports on the Kingdom’s first COVID-19 case, a Saudi patient who had returned from Iran.
Two days later, the Kingdom identified its second patient, another Saudi citizen who had traveled with the first case. Both had failed to disclose that they had been in Iran.
The following day, the Kingdom publicly rebuked Tehran for allowing Saudi citizens to enter the country during the outbreak, and urged any citizens who were still in Iran or who had returned from there recently to come forward within 48 hours, promising immunity from prosecution.
But by then the genie was already out of the bottle.
By March 9, 2020, the Kingdom had recorded 15 confirmed cases of COVID-19, seven of whom had come from Iran and three from Iraq.
It was, in other words, apparent early on that Iran would be the weak link in the region’s defenses against COVID-19. By March 2, the day Saudi Arabia had its first case, Tehran had already admitted to 978 cases and 54 deaths. By the time the Kingdom’s second case emerged two days later, Iran’s caseload had more than doubled to 2,336, with 77 declared deaths.
Even that, it seems, may have been a wilful gross underestimate of the true impact of the disease. Internal Iranian government documents leaked to the BBC’s Persian service at the beginning of August 2020 revealed that the true scale of the pandemic in the country at that point was almost twice as bad as Tehran admitted.
On March 25, just over three weeks after the Kingdom’s first case, COVID-19 claimed its first victim in Saudi Arabia, a 51-year-old Afghani who died in Madinah.
After that, the toll of cases and deaths began to climb.
The number of new daily cases in Saudi Arabia would see three distinct peaks in 2020, hitting a high on June 17, when 4,919 infections were reported in one day.
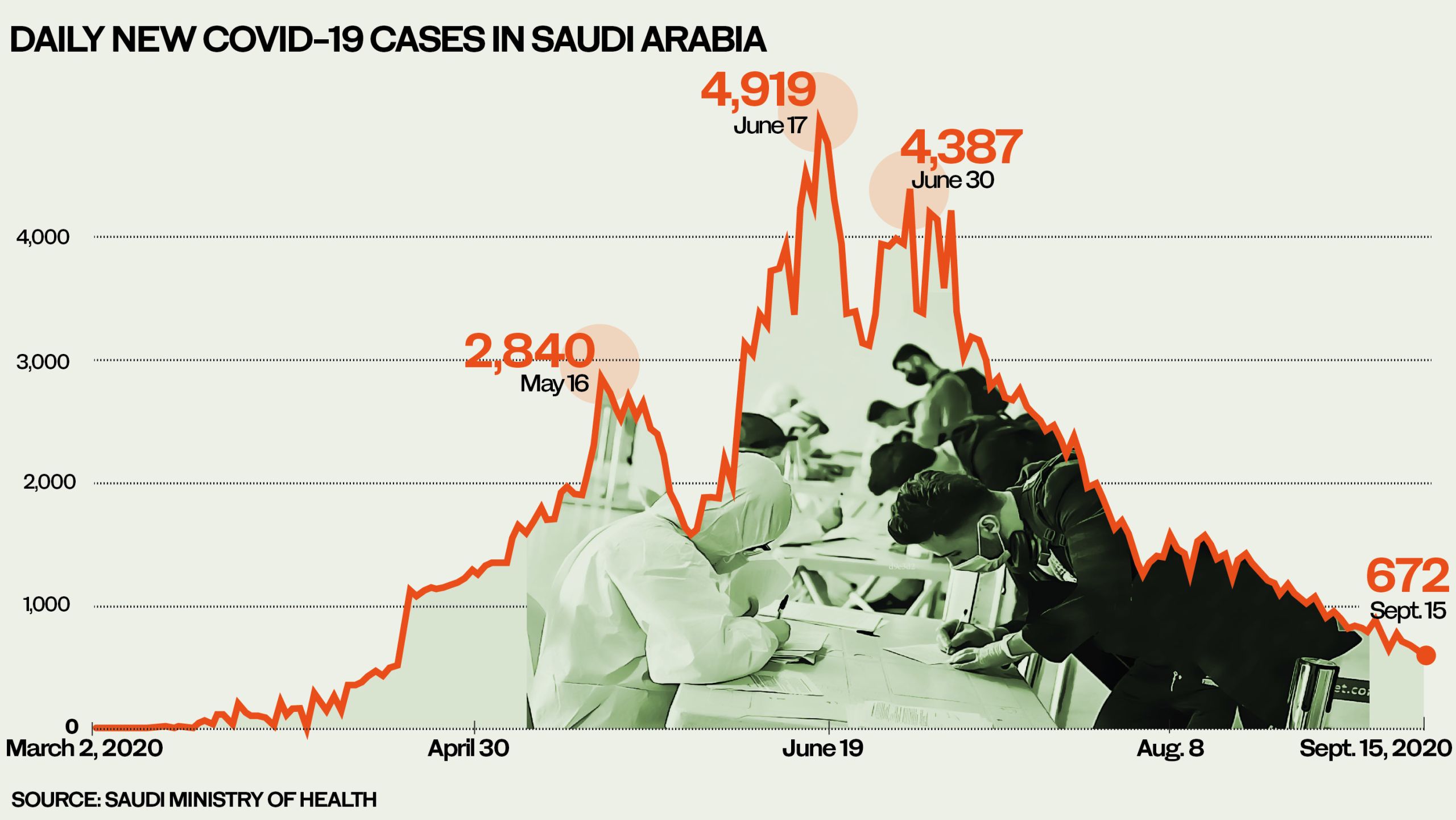
In the first year of the pandemic reported daily cases in Saudi Arabia would see three peaks, with a high on June 17.
Many feared Saudi Arabia was on the brink of losing control of the pandemic. There would be a third uptick, with 4,387 cases reported on June 30, but the record high of 4,919 cases would not be seen again that year.
Slowly, but surely, Saudi Arabia was winning the battle. After July 6, the number of daily cases began to fall steadily, dropping below 1,000 on Aug. 29 to 987 — a figure not seen since the middle of April.
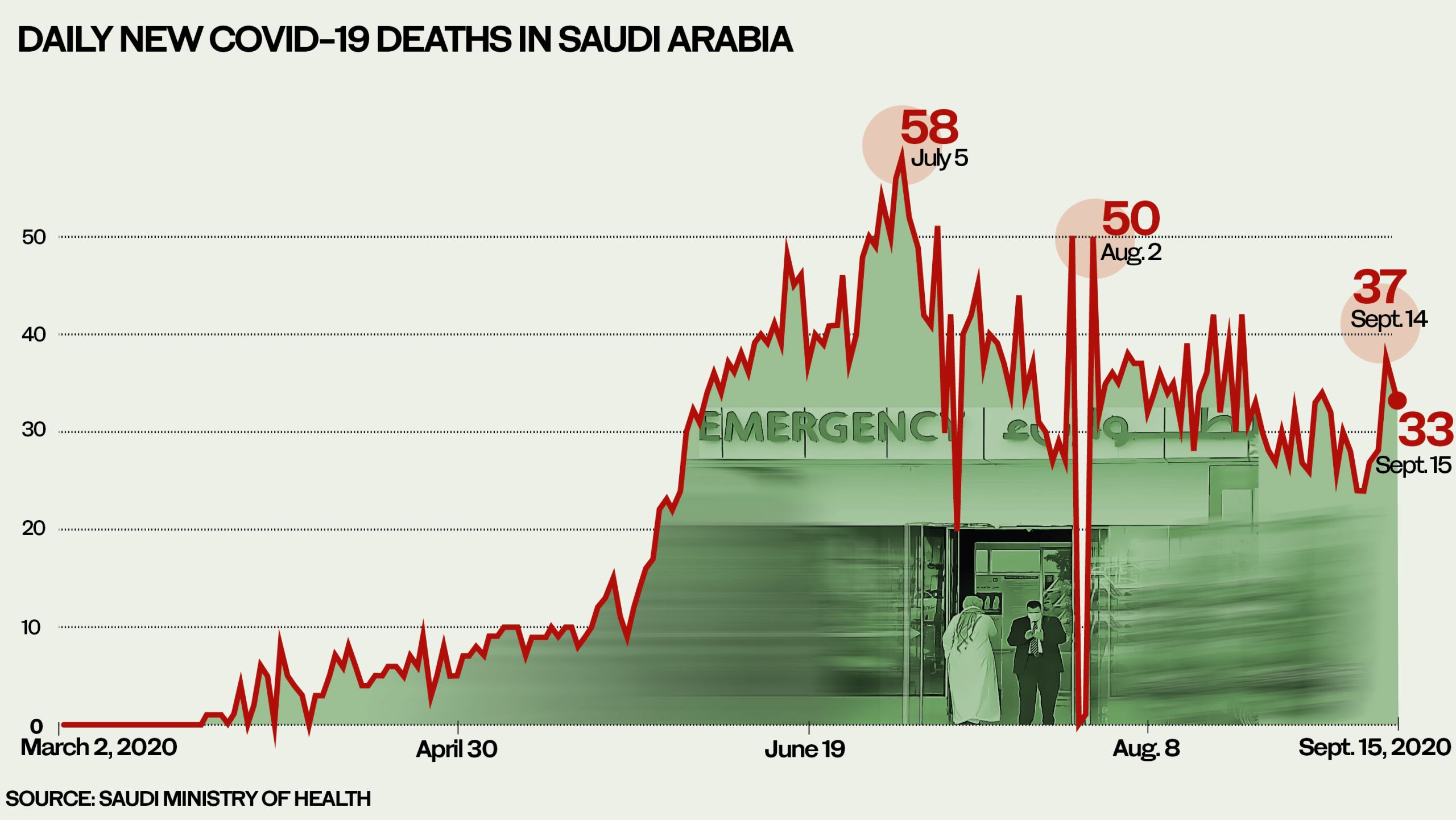
The number of daily deaths in 2020 peaked at 58 on July 5, falling to 33 by Sept. 15.
Toward the end of 2021, the entire world was flat-footed for a while by the emergence of the omicron variant, and Saudi Arabia was no exception.
After months of recording only a handful of daily new infections, cases suddenly spiked at the end of December, hitting a record 5,928 on Jan. 19, 2022. By now, however, vaccines were in play and, besides, while being more easily spread, omicron would prove to be less deadly.
From a peak of 58 deaths on July 5, 2020, since the end of October 2021 there have never been more than three or four deaths a day in the Kingdom, and more often none.
But as Saudi Arabia emerges from the worst days of the pandemic and gradually returns to normal, it is time to count the cost.
By June 13, 2022, there had been a total of 780,135 cases of COVID-19 in the Kingdom, and 9,176 lives had been lost. The global toll by then was 536 million cases and almost 6.31 million deaths.
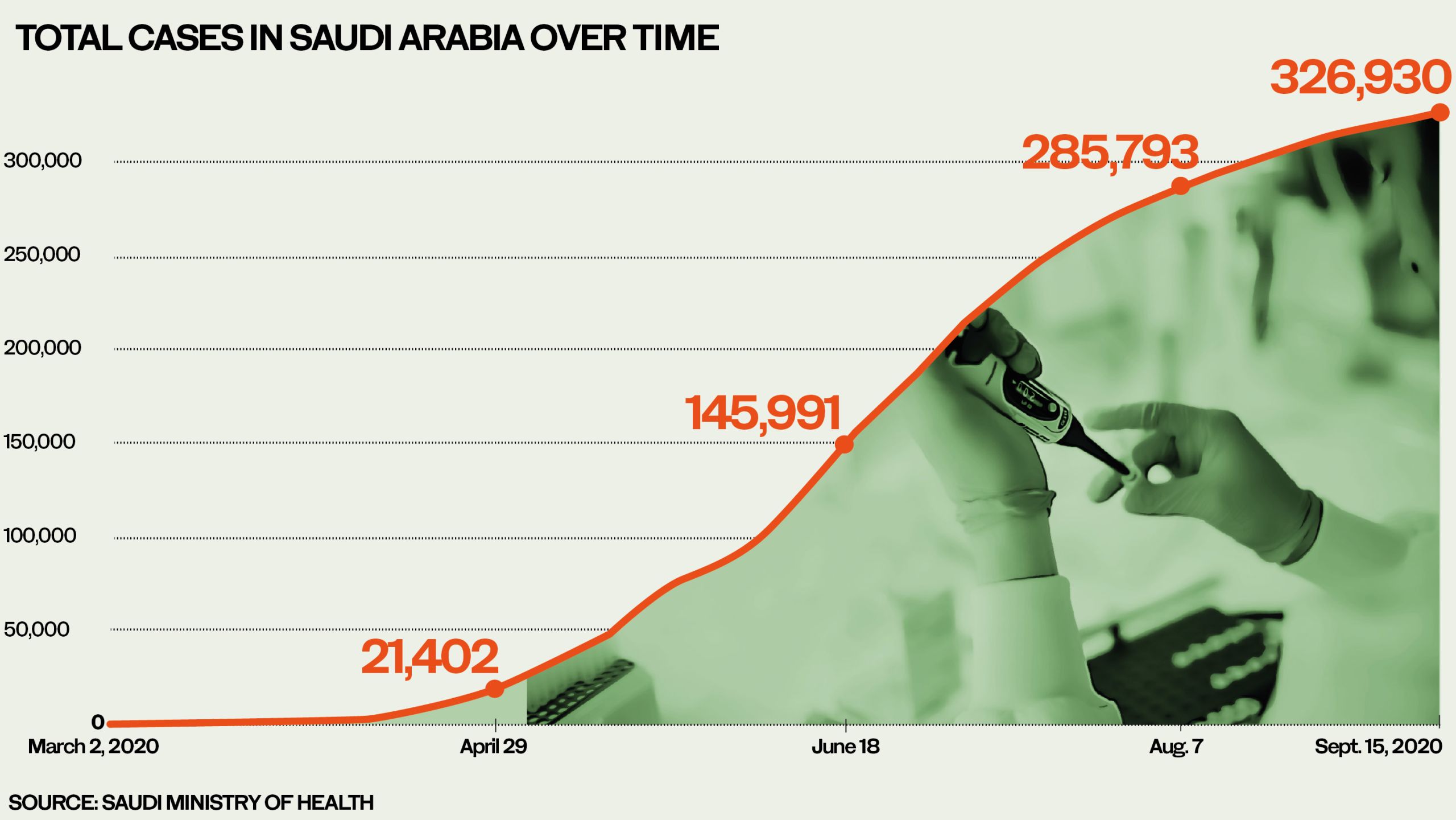
By Sept. 15, 2020, there had been a total of 326,930 cases in the Kingdom. The global toll by then was 29.7 million cases.
It is now possible to compare Saudi Arabia’s performance in the battle against COVID-19 with that of other countries. The best resource for doing so is Our World in Data, a collaboration between researchers at Oxford University’s Oxford Martin Programme on Global Development and the nonprofit organization Global Change Data Lab, and analysis of this data by the Worldometer initiative.
Looking only at total numbers of cases and deaths gives a distorted impression. With 780,135 cases by June 14, 2022, Saudi Arabia is the 77th worst-affected country in the world. On a table measuring global mortality, its 9,176 deaths put it in 66th position overall.
But in isolation these figures are misleading; it is important to look at the number of cases, deaths and other statistics per head of population.
With a total of only 21,750 cases per 1 million population as of June 14, the Kingdom was in 161st position in the world, rather than 66th, and by this measure outperformed all the other GCC states by a considerable distance.
Bahrain had 328,749 cases per million, Kuwait had 144,818, Qatar 132,907, the UAE 90,901 and Oman 72,728.
But another factor has to be taken into account — the sheer size of Saudi Arabia compared with other GCC states and the fact it shares lengthy borders with no fewer than seven countries.
With a population of almost 35 million, spread over a vast area, the Kingdom has faced a task far more daunting than other, smaller GCC states: The UAE (population 9.9 million), Oman (5.1 million), Kuwait (4.27 million), Qatar (2.8 million) and Bahrain (1.7 million).
The number of deaths should also be seen in relation to population size. The Kingdom’s total of 9,176 deaths by June 14 represents a rate of 256 fatalities per million head of population, placing Saudi Arabia well below the global average of 812. By this measure, it was performing better than a basket of 147 other countries, including the UK, Canada and the US, and a host of European states.
These figures put the Kingdom on a par with Qatar (241 deaths per million) and the UAE (228), but far ahead of Kuwait (583), Oman (795) and Bahrain (820).
Nevertheless, when the all-important post-crisis analysis takes place, answers must be found to some difficult questions. One of these relates to the Kingdom’s case fatality rate (CFR) in the first year of the pandemic. This is the ratio between the number of cases and deaths — in other words, the percentage of people who contracted the disease and went on to die from it.
As our graph shows, after an initial rapid climb and spike on April 7 2020, the Kingdom’s CFR improved dramatically, even as that of Kuwait and the UAE was still climbing.
While Saudi Arabia’s case fatality rate of 1.3 percent by September 2020 was the worst among Gulf Cooperation Council countries, it compared highly favorably with the global average of 3.2 and with that of a range of countries, including the UK (11.2) and the US (3).
By the end of May, however, the situation had begun to reverse. As of Sept. 15, 2020, Saudi Arabia’s CFR of 1.3 percent — meaning that more than one out of every 100 COVID-19 patients had died — was the worst in the GCC (compared with 0.9 in Oman, 0.6 in Kuwait, 0.5 in the UAE, 0.4 in Bahrain and 0.2 in Qatar).
Apart from the initial improvement, the Kingdom’s case fatality rate would remain the highest in the GCC throughout the pandemic. On June 13 2022, it was 1.18 percent, which was the global average and the same rate as in the US, but higher compared with Oman (1.09), Kuwait (0.4), the UAE and Bahrain (0.25) and Qatar (0.18).
According to Al-Ghamdi, deputy CEO of the Saudi Center for Disease Prevention and Control, most of the differences in CFR rates could be attributed to variations in population characteristics.
“For example, the percentage of elderly people in Western countries is much higher than the percentage in Saudi Arabia, and we know now from all evidence that the elderly are more at risk of complications from COVID-19, and that the risk of dying is high among them,” he said.
Similarly, Al-Ghamdi added, “in comparison with other countries in the region, the same will apply. We have different percentages of chronic diseases, and that will affect the outcome. But in general, the outcome of COVID-19 cases in Saudi Arabia is among the best in the world.”
Credit for this, he said, must be given to the royal decree that “enabled everybody in Saudi Arabia, whether they are Saudi or non-Saudi, whether they are legal or illegal, to access health care services if they are positive for COVID-19. This has provided a huge advantage for Saudi Arabia and has led to a very good outcome.”

On March 3, 2000, Arab News reports on the Kingdom’s first COVID-19 case, a Saudi patient who had returned from Iran.
On March 3, 2000, Arab News reports on the Kingdom’s first COVID-19 case, a Saudi patient who had returned from Iran.

In the first year of the pandemic reported daily cases in Saudi Arabia would see three peaks, with a high on June 17.
In the first year of the pandemic reported daily cases in Saudi Arabia would see three peaks, with a high on June 17.
The number of daily deaths in 2020 peaked at 58 on July 5, falling to 33 by Sept. 15.
The number of daily deaths in 2020 peaked at 58 on July 5, falling to 33 by Sept. 15.
By Sept. 15, 2020, there had been a total of 326,930 cases in the Kingdom. The global toll by then was 29.7 million cases.
By Sept. 15, 2020, there had been a total of 326,930 cases in the Kingdom. The global toll by then was 29.7 million cases.

While Saudi Arabia’s case fatality rate of 1.3 percent by September 2020 was the worst among Gulf Cooperation Council countries, it compared highly favorably with the global average of 3.2 and with that of a range of countries, including the UK (11.2) and the US (3).
While Saudi Arabia’s case fatality rate of 1.3 percent by September 2020 was the worst among Gulf Cooperation Council countries, it compared highly favorably with the global average of 3.2 and with that of a range of countries, including the UK (11.2) and the US (3).
Watch what the streets of Saudi Arabia looked like as it joined the world in a lockdown to prevent the spread of COVID-19 — a haunting yet beautiful stillness.
What Saudi Arabia did to keep COVID-19 at bay


The new COVID-19 Follow-up Committee, formed to monitor and coordinate the national response to the disease in Saudi Arabia, held its first meeting on Feb. 1. Just how seriously the Kingdom was taking the new threat was reflected in the broad membership of the group, chaired by Dr. Tawfiq bin Fawzan Al-Rabiah, then the country's health minister.
Around the table were representatives from 13 ministries: Health, defense, energy, interior, National Guard, foreign affairs, finance, media, commerce and investment, Hajj and Umrah, education and tourism. Also present were the General Authority of Civil Aviation, Saudi Red Crescent Authority, Saudi Food and Drug Authority, General Authority of Customs, and the Saudi Center for Disease Prevention and Control.
From the outset, as the WHO would shortly acknowledge, Saudi Arabia was determined to be as ready as possible to confront the horror that was edging ever closer to its borders.
For Al-Ghamdi, the extent to which the Kingdom has weathered the COVID-19 storm was a product of effective leadership and a nationally coordinated response.
“It was a very good exercise for the government and for the public health and healthcare system to see the gaps and to address them immediately,” he said. Furthermore, “it has given us a chance to reflect in the coming months and years and to implement any necessary changes that will put Saudi Arabia in the best position to meet any future challenges to the system.”
In a statement on March 25, 2020, Dr. Ahmed Al-Mandhari, the WHO’s regional director for the Eastern Mediterranean, praised the Kingdom’s rapid response. Its experience with MERS had not been forgotten, he said, and the country was “also drawing from its unique expertise in managing mass gatherings and emergency preparedness during the annual Hajj pilgrimage.”
On March 17, 2020, Saudi Arabia temporarily closed all places of worship but for the Two Holy Mosques in Makkah and Madinah. Three days later, these too were shut. (AFP)
At its 10th meeting, on Feb. 29, 2020, the COVID-19 committee cautiously noted that, even as the wider world was reeling under the impact of over 88,000 cases and almost 3,000 deaths, Saudi Arabia still remained virus-free.
But in the span of two days, all that would change.
It took a little over two months for COVID-19 to make its way to Saudi Arabia. By the time the Kingdom had its first case on March 2, the world had recorded 91,000 cases and 3,118 deaths.
The majority of those cases were still in China, but it was already clear that efforts to contain the virus within that country had failed; more than 10,000 infections and 172 deaths had already been recorded beyond China’s borders.
From the beginning, Saudi authorities realized that the tidal wave that was rapidly engulfing the world would inevitably sweep through the Kingdom, but thanks to the two-month period during which the virus was held at bay, they had time to plan for the worst.
“We were luckier than many other countries because our cases started a little bit later,” said Dr. Hani Jokhdar, deputy minister for public health, speaking in August at the virtual Riyadh Global Digital Health Summit. “This gave us a small opportunity to develop our systems, watching and observing what was happening in the rest of the world.”
Saudi Arabia’s breathing space was not down solely to luck. On Jan. 28 2020, more than a month before the Kingdom saw its first case, the Ministry of Health had launched a public information campaign. At the same time, plans were being laid for the introduction of widespread testing, the tracing of contacts of confirmed cases and the introduction of systems for quarantining.
Saudi Arabia took early precautions to confront the pandemic, including launching awareness campaigns, closing public venues, and securing laboratory testing. (AFP)
It was not a moment too soon. On Feb. 2, 10 Saudi students were evacuated from Wuhan and flown to Riyadh on a private aircraft sent by the government. All tested negative for COVID-19 but were nevertheless quarantined for two weeks.
But the disease, helped by still largely unrestricted global air travel, was moving fast. On Feb. 4, a day on which China’s number of infections passed 20,000, with 426 deaths, the WHO was still failing to recommend that countries impose travel restrictions.
In fact, on Feb. 4, Dr. Tedros Adhanom Ghebreyesus, the WHO’s director-general, took the extraordinary step of urging countries not to ban flights from Wuhan, saying this would “have the effect of increasing fear and stigma, with little public health benefit.”

WHO Director-General Tedros Adhanom Ghebreyesus wears a mask after leaving a ceremony in Geneva. King Salman authorized $10 million to help the WHO in Yemen combat COVID-19. (AFP)
Regardless, two days later, on Feb. 6, 2020, Saudi Arabia banned citizens and residents from traveling to China. It would be March 11 before the WHO finally declared a pandemic, a state of affairs already blindingly obvious to the 114 countries which by then were in the grip of the outbreak.
As governments around the world reacted to the threat with little cohesion, it seemed remarkable that the Kingdom had kept the virus at bay for as long as it did. It was the last of the six GCC states to be hit.
As governments around the world reacted to the threat with little cohesion, it seemed remarkable that the Kingdom had kept the virus at bay for as long as it did. It was the last of the six GCC states to be hit.
Throughout February, as health and security teams were mobilized and trained, a series of measures were taken in response to the rapidly evolving global picture.
Some of those steps were reported in a paper published in the Saudi Pharmaceutical Journal in May, with the title “Importance of Early Precautionary Actions in Avoiding the Spread of COVID-19: Saudi Arabia as an Example.”
Saudi Arabia, wrote the authors from the Saudi Food and Drug Authority, King Saud University, King Khalid Hospital, and the Regional Drug Information and Pharmacovigilance Center in Tabuk, “was one of the countries that took very early precautionary actions … before any cases occurred and before the WHO declared that COVID-19 was an epidemic.”
From the outset of the pandemic, precautionary measures had been tightened at health surveillance centers at all ports of entry, with all passengers coming from countries stricken by COVID-19 screened and isolated and their health monitored.
One aspect of the nation’s preparedness — its self-sufficiency in essential medical equipment throughout the crisis — was covered by Arab News, which on Aug. 12 reported that about 50 industrial units in the Kingdom had been busy producing essential medical goods. One of them, Enayah, even had sufficient capacity to export its products to GCC neighbors, other Arab countries and the EU.
Saudi Arabia was also one of the first countries to set up secure laboratory testing for COVID-19. On March 5, testing was introduced for anyone with symptoms. By July 13, more than 2 million COVID-19 tests had been carried out, and by Aug. 31 the total had exceeded 5 million.
On Feb. 19, citizens and residents were asked to postpone travel to Singapore, which had recorded 80 cases. It was the beginning of a series of travel restrictions culminating on March 15, when the Kingdom became only the second GCC state to impose a ban on all international flights. Simultaneously, shipping services with 50 countries, excluding cargo-carrying vessels, were suspended, and on March 21 bans were imposed on internal air, train and bus travel.
On Feb. 27, 2020, Saudi Arabia took the unprecedented step of suspending Umrah visas for foreign pilgrims.
On March 5, dozens of events, including the Riyadh International Book Fair and Saudi Arabian International Horse Festival, were canceled. Three days later, the entire population of Qatif, the city in the Eastern Province where most of the Kingdom’s early cases had emerged, was placed under quarantine, and schools and universities across the nation were closed. Bans on gatherings and wedding ceremonies would follow on March 13.3.

On March 8, 2020, Saudi authorities announced the closure of all public and private universities and schools across the country. (AFP)
Focused though it was on its own looming crisis, on March 9 the Kingdom responded to the WHO’s plea for countries to do more to combat COVID-19 by donating $10 million to the organization’s regional fighting fund. At home, SR50 billion ($13 billion) was allocated to support the Kingdom’s banking sector, financial institutions and small-to-medium businesses.
On March 19, 2020, demonstrating that the entire leadership of Saudi Arabia was focused on preparing for the pandemic, King Salman gave a rare public address on television, appealing to the nation’s “heightened sense of collective responsibility.”
The Kingdom, he said, “continues to take all precautionary measures to confront this pandemic and limit its effects. We depend on the aid of God Almighty, then on deploying our full capabilities, supported by your strong determination in the face of adversity.”
He added: “The strength, steadfastness and determination that you have demonstrated during this difficult phase, and your full cooperation with relevant government agencies, are the most important contributing factors and pillars of the success of the state’s efforts.”
On March 23, the king authorized a further $10 million to provide the WHO in Yemen with essential equipment and supplies, and Saudi Arabia began airlifting medical equipment and supplies from the WHO’s logistics hub in Dubai to Aden to boost Yemen’s readiness for COVID-19.
“This funding will help the WHO intensify its efforts as it takes regional and global action to combat the spread of the disease,” said Al-Mandhari, the WHO’s regional director.
On March 22, King Salman ordered a 21-day curfew from 7 p.m. to 6 a.m. across the whole of the country. The only exceptions would be for workers in vital industries, including food shops, pharmacies and medical services, and those working in water, energy and transportation. Three days later, the curfew in Makkah and Madinah was extended to start at 3 p.m.
It was also clear that, in the interests of preventing the spread of the disease, nothing should be allowed to stand in the way of any citizen or resident seeking medical help, and on March 30, King Salman ordered that all COVID-19 patients in the Kingdom should be treated free of charge.
The order applied to everyone, including violators of residence, labor or border security laws, who “shall all be treated at the public and private hospitals and healthcare centers free of charge, and without any legal liability whatsoever.”
On April 6, as the number of cases grew in specific regions, a 24-hour curfew was imposed on the cities of Riyadh, Tabuk, Dammam, Dhahran and Al-Hofuf, as well as the governorates of Jeddah, Taif, Qatif and Alkhobar. Residents were allowed to leave their homes between 6 a.m. and 3 p.m., but only for essential needs within their own areas.
The following day, April 7, Al-Rabiah, as health minister, warned that the rate at which COVID-19 infections increased in Saudi Arabia over the coming weeks would depend “primarily on the cooperation of all, and their commitment to the instructions and guidelines issued by the authorities.”
The state was doing its part. A total of SR8 billion had already been allocated to the fight against the virus, and following a virtual meeting on April 6, Crown Prince Mohammed bin Salman approved an additional cash injection of SR7 billion. Over the next three months, more than 2,800 intensive care unit beds were added, increasing the Kingdom’s stock by 30 percent.
But some individuals, said Al-Rabiah, were “not dealing seriously with the pandemic, and (were) not complying with the measures banning close contact and gatherings.”
Al-Rabiah also revealed the results of four studies that had been carried out by epidemiologists, predicting that the total number of cases over the next few weeks could range from at least 10,000 to 200,000. “Noncompliance,” he added, “will lead to a huge increase.”
The message got through. As revealed at the ministry’s daily COVID-19 briefing on July 2, Assistant Minister of Health Dr. Mohammed Al-Abdulaali noted that it had taken 90 days, instead of the predicted 30, to reach the 200,000 cases. The Kingdom, he said, had successfully bought time “to better manage the crisis.”
Along with its GCC neighbors, Saudi Arabia on April 26 temporarily relaxed daytime restrictions ahead of the start of Ramadan, allowing people everywhere except Makkah and a few isolated districts to leave their homes between 9 a.m. and 5 p.m. each day. On May 13, the 24-hour curfew was reimposed on the whole country for the duration of the Eid Al-Fitr holiday.
At the end of May, the Ministry of Interior announced precautionary measures and preventive protocols for several sectors in preparation for a relaxing of the nationwide curfew from June 21. Restrictions remained in place, however, for religious pilgrimages, international travel and gatherings of more than 50 people.
Speaking at a press conference, Minister of Finance Mohammed bin Abdullah Al-Jadaan, also the acting minister of economy and planning, said the gradual lifting of curfews represented “a new stage in the face of the global pandemic crisis and toward a gradual return to economic activities in the Kingdom to its normal levels.”
As Al-Rabiah explained at the Riyadh Global Digital Health Summit in August, technology — some new, some already in use and rapidly adapted — would be the main weapon in the Kingdom’s battle against COVID-19.
“During the Kingdom’s presidency of the G20 and prior to the emergence of the pandemic, we have introduced pandemic preparedness and digital health as key priorities,” he told the summit.
The emphasis on digital health, Al-Rabiah said, “was critical as it plays a fundamental role in supporting health emergency management by strengthening existing response mechanisms.” Digital tools, he added, “also enable innovative, equitable access to health services, data sharing and improved coordination.”
Also speaking at the summit, Jokhdar, the deputy minister for public health, described how, as Saudi Arabia had watched and waited for the inevitable arrival of COVID-19, “(it) saw countries with good healthcare systems hit by numbers of cases that exceeded their capacity to handle public health strategy and defense mechanisms.”
The lesson quickly taken on board was that existing public-health technology, designed primarily for use in hospital settings, “was not up to allowing countries to handle such a big pandemic.”
At that point, said Jokhdar, ministers took a long hard look at Saudi Arabia’s own preparedness. “We thought, OK, let’s set up our team, let’s look at our technology and how we can benefit from what we already have on the ground.
“We have our command and control center, and our emergency operations center functioning for a few years. Let’s ask them what they want in order to make our technology team ready to help us with this pandemic if it happens in Saudi Arabia.
“Then we looked at our National Health Command Center dashboard, which was in preparation for the past two years and launched about a year ago, focused on hospital and primary health care operations, and we asked: Can we utilize that, can we transform that into something else?”
The answer was yes.
In a remarkably short period, the NHCC, which had been set up primarily to monitor the day-to-day operations of hospital and primary healthcare facilities, was adapted to allow ministry staff to keep tabs on every development in the battle against COVID-19. It became “an early-warning system of great added value.”
Feeding into the NHCC, and informing all the decisions taken on a daily basis in the battle against the virus, was a continuous stream of data harvested by a series of apps and other digital systems, some already in existence and adapted for the crisis, others developed quickly to deal with it.
These included Mawid, a centralized appointments-booking system for primary health care, and Seha, an app allowing people to consult a doctor by text, telephone or video conference, book COVID-19 test appointments, and carry out COVID-19 self-assessments.
The Tabaud app allowed users to know if they had been in contact with anyone confirmed to be positive for COVID-19, while Takasi was an online platform allowing health care workers to enter patient data and organize mass testing, active target surveillance and contact tracing.

A nurse checks a patient’s temperature at a mobile clinic in Makkah on April 7, 2020. Through a series of apps, the Kingdom was able to facilitate health care for its residents. (AFP)
Launched on April 11, 2020, Tetamman (“Rest Assured”) was developed as a smartphone “digital caring system” allowing users to easily access accurate educational material and upload their symptoms — prompting a call, if necessary, from a 937 adviser. When it came to mass testing, Tetamman proved to be priceless, offering people access to drive-through testing stations set up by the ministry in 17 cities.
The number of new daily cases peaked in Saudi Arabia on June 17, when a record 4,919 were reported. A month later, as the nation made what officials described as a “cautious return to normality,” it was clear that the number was dropping almost daily. At the daily briefing on July 21, Assistant Minister of Health Al-Abdulaali attributed the fall in cases to “the involvement of all people.”
Judging objectively how any nation has coped with the pandemic is fraught with confounding social, cultural and economic factors and a complex, ever-changing global picture, all of which is hard to factor into any assessment and which make comparisons with other nations especially problematic.
That, however, was the task taken on by researchers at the Blavatnik School of Government at the University of Oxford, who at the beginning of the crisis set out to monitor and document the policy responses to COVID-19 of governments around the world.
A team of more than 100 Oxford University students and staff from every part of the world has been painstakingly collecting publicly available information on 17 indicators of government responses, including containment and closure policies, such as school closures and restrictions on movement, and economic and health-system policies, such as testing regimes.
The result is the Oxford Coronavirus Government Response Tracker, in which the higher the score, the stricter a government’s response is deemed to have been.
It is reassuring to note that throughout the pandemic, Saudi Arabia’s response has been rated as consistently tougher than that of many other nations, including the UAE, UK and US.
In countries where governments have hesitated to act, or allowed internal politics to derail public health strategies, COVID-19 has run rampant. As a comment article on Euronews put it on April 3, “while some governments have been paralyzed by the confusion, fear and uncertainty surrounding the pandemic, Riyadh has taken tough decisions for the greater good — and continues to do so.”
In the Kingdom, added the website, there had been “a mass mobilization of government, media and civil society to create the kind of overnight awareness, focus and solidarity that is essential during a global pandemic … mobilization that is sorely lacking in some Western capitals.”
Saudi Arabia, of course, has not escaped the curse of the virus — no country has. But the truly catastrophic experience of many nations, such as the US and the UK, has shown that without the sort of decisive governance exercised in the Kingdom this year, the price paid by the citizens of Saudi Arabia could have been much higher.
And, on Sept. 15, as the number of daily new cases in Saudi Arabia continued to tumble, hitting a low not seen for five months, the Kingdom made a hugely symbolic announcement, raising the prospect of a full return to normality in the new year.
Six months after travel restrictions were first imposed, Saudi Arabia was partially lifting the suspension of international flights, aiming to end all restrictions on travel by land, sea and air after Jan. 1, 2021.

On March 17, 2020, Saudi Arabia temporarily closed all places of worship but for the Two Holy Mosques in Makkah and Madinah. Three days later, these too were shut. (AFP)
On March 17, 2020, Saudi Arabia temporarily closed all places of worship but for the Two Holy Mosques in Makkah and Madinah. Three days later, these too were shut. (AFP)

Saudi Arabia took early precautions to confront the pandemic, including launching awareness campaigns, closing public venues, and securing laboratory testing. (AFP)
Saudi Arabia took early precautions to confront the pandemic, including launching awareness campaigns, closing public venues, and securing laboratory testing. (AFP)

WHO Director-General Tedros Adhanom Ghebreyesus wears a mask after leaving a ceremony in Geneva. King Salman authorized $10 million to help the WHO in Yemen combat COVID-19. (AFP)
WHO Director-General Tedros Adhanom Ghebreyesus wears a mask after leaving a ceremony in Geneva. King Salman authorized $10 million to help the WHO in Yemen combat COVID-19. (AFP)

On March 8, 2020, Saudi authorities announced the closure of all public and private universities and schools across the country. (AFP)
On March 8, 2020, Saudi authorities announced the closure of all public and private universities and schools across the country. (AFP)

A nurse checks a patient’s temperature at a mobile clinic in Makkah on April 7, 2020. Through a series of apps, the Kingdom was able to facilitate health care for its residents. (AFP)
A nurse checks a patient’s temperature at a mobile clinic in Makkah on April 7, 2020. Through a series of apps, the Kingdom was able to facilitate health care for its residents. (AFP)
An extraordinary Hajj, free of COVID-19

'Every precaution was taken, from screening and isolating pilgrims prior to Hajj to fitting them with the electronic bracelets.'


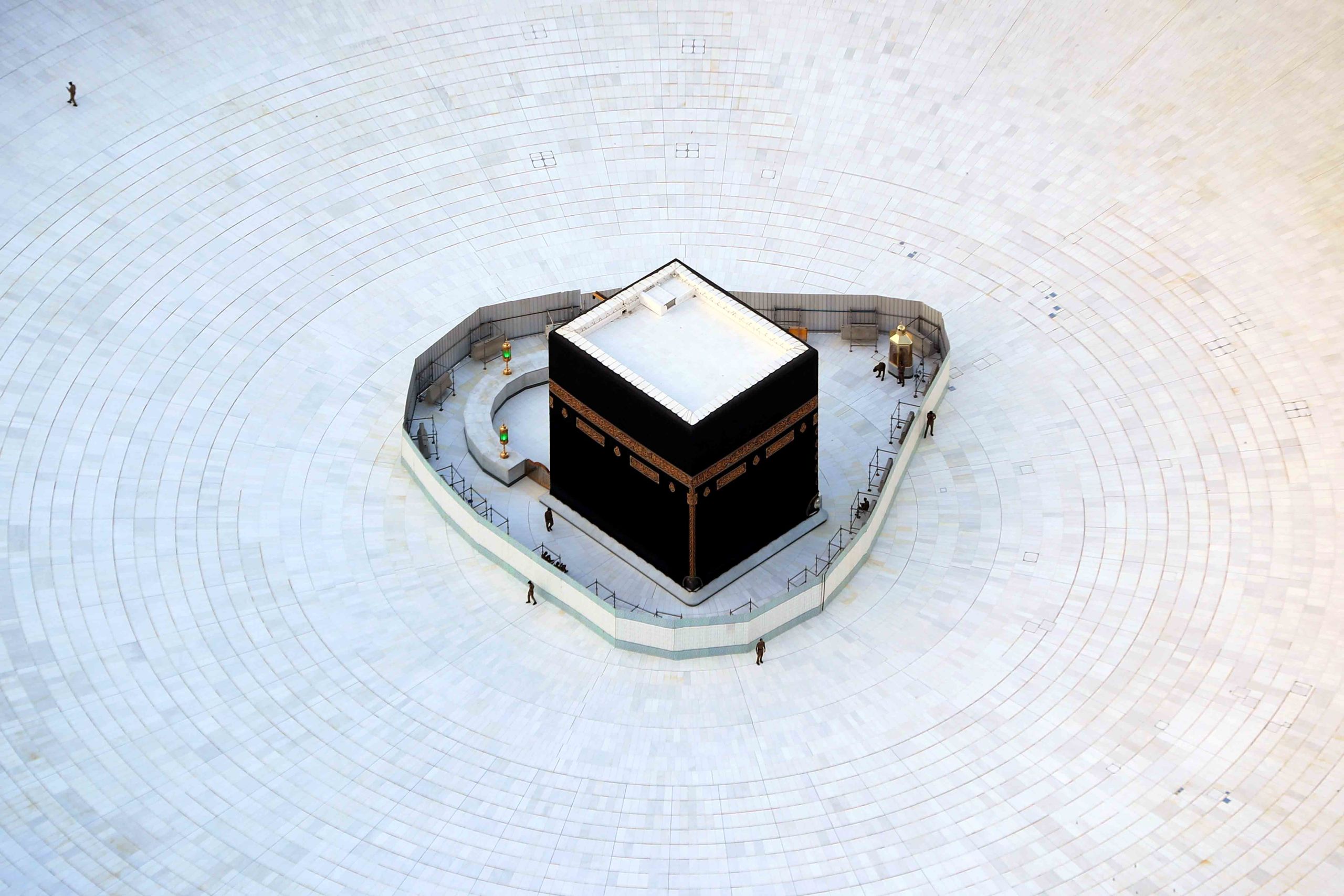
Of all the extraordinary images beamed around the world from the unprecedented Hajj in 2020, it was the time-lapse footage of pilgrims circumambulating the Kaaba with carefully choreographed, socially distanced precision that best captured the spirit of Saudi Arabia’s determination to tackle the pandemic effectively, efficiently and on its own terms.
For months after the virus first emerged, it was uncertain that Hajj would go ahead, even in the much-reduced form that it would eventually take.
What quickly became clear, however, was that with responsibility for the millions of pilgrims who visit each year, and by extension for the well-being of the nations from which they came, Saudi Arabia was not going to take any chances on their behalf.
On Feb. 27, before a single case of COVID-19 had been detected in the Kingdom and while the WHO was still urging countries not to ban flights from Wuhan, Saudi Arabia announced that it was suspending overseas visitors’ visas for Umrah, the lesser pilgrimage, and closing the holy sites to foreigners.
On March 17, even as other Muslim countries hesitated to act, the Kingdom took the unprecedented, but necessary, step of temporarily closing all places of worship but for the Two Holy Mosques in Makkah and Madinah. Three days later, these, too, were shut.
Such bold decisiveness was in contrast to Iran’s perverse decision to shut its mosques but keep open holy sites that attract millions of pilgrims every year in the cities of Qom and Mashhad. Early in March, disturbing footage emerged on social media of Shiite pilgrims touching, kissing and even licking shrines.
In Saudi Arabia, the decision on whether to go ahead in July with Hajj, an event of vital importance to Muslims everywhere, could not be rushed.
In Saudi Arabia, the decision on whether to go ahead in July with Hajj, an event of vital importance to Muslims everywhere, could not be rushed.
Much was at stake. For Hajj in 2019, 2.5 million pilgrims had converged on Makkah. Of these, 634,000 were from within the Kingdom itself, and it was clear that welcoming a similar number in 2020 would heighten the risk of the disease spreading like wildfire.
Even worse, more than 1.85 million pilgrims had come from overseas, including 60 percent from Asian countries and 22 percent from other Arab states.
The prospect of potentially sending large numbers of pilgrims home with the virus to dozens of countries around the world was unthinkable and, in the end, Saudi Arabia settled on a historic and symbolic compromise.
Hajj would go ahead in 2020, but with only 1,000 representative pilgrims, selected from nationals and foreigners already resident in the country.
Even 1,000 was a challenging number at a time when the entire world, including Saudi Arabia, was working hard to limit transmission of the disease by restricting social gatherings. But the way the complex series of Hajj rituals was managed by the authorities earned praise from across the globe.
As Al-Rabiah, the health minister, explained at the Riyadh Global Digital Health Summit in August, it was the use of digital tools, “along with the implementation of exceptional health and safety measures,” that had “assisted (Saudi Arabia) in successfully navigating what is typically one of the largest religious gatherings in the world under extraordinary circumstances.”
“Pilgrims arriving in the holy cities were electronically tagged with bracelets designed to monitor and record their health status, and track individuals quarantined upon their return home,” Al-Rabiah explained. “And as a result, we have been very fortunate to have had zero cases of COVID-19 during Hajj this year.”
Every precaution was taken, from screening and isolating pilgrims before Hajj to fitting them with the electronic bracelets. Groups of 50 worshippers were each led by a medically qualified guide. Face masks were mandatory, only pre-bottled Zamzam water could be consumed, and even the pebbles used for the symbolic stoning of the devil, normally collected from the ground at Muzdalifah by the pilgrims themselves, were gathered beforehand, sterilized and issued in bags.
As a result, not a single case of COVID-19 emerged during Hajj, a public-health victory for the state that belonged also to the pilgrims, whose behavior and adherence to the new rules was exemplary.















By observing rigorous precautionary measures, 1,000 representative pilgrims were able to proceed with Hajj in 2020. (All images from Saudi Ministry of Media)
By observing rigorous precautionary measures, 1,000 representative pilgrims were able to proceed with Hajj in 2020. (All images from Saudi Ministry of Media)

New rules stipulated face masks.
New rules stipulated face masks.

Grounds were sterilized.
Grounds were sterilized.

Medically qualified guides led groups.
Medically qualified guides led groups.

Strict social distancing measures were put in place.
Strict social distancing measures were put in place.

Pilgrims were screened and isolated.
Pilgrims were screened and isolated.

Electronic bracelets were distributed.
Electronic bracelets were distributed.
Moving forward with global partners


As the holder of the presidency of the G20 throughout most of 2020, Saudi Arabia was at the forefront of initiatives to ensure that the global battle against the virus was better coordinated, effective and fair — and that the world is better prepared for the next onslaught.
As early as March 18, 2020, the Kingdom called for an extraordinary virtual summit of G20 leaders “to put forward a coordinated set of policies to protect people and safeguard the global economy.”
At the meeting, hosted by King Salman a week later, presidents, prime ministers and heads of state committed to spending $5 trillion on measures to combat the infection, as well as the economic and financial fallout.
In May, 2020, Saudi Arabia helped to organize a global donor conference hosted by European leaders that raised more than $7 billion toward efforts to find a COVID-19 vaccine. And in July, the Kingdom hosted an emergency virtual meeting of G20 finance ministers and central bankers, who pledged “to continue to use all available policy tools to safeguard people’s lives, jobs and incomes, support global economic recovery, and enhance the resilience of the financial system” in the battle to help the world recover from the economic impact of the pandemic.
The Kingdom swiftly introduced one of the world’s most effective vaccine regimes — by June 14, 2022, a total of 66,544,534 doses had been administered. But drugs are only part of a country’s armory when it faces a pandemic, and Saudi Arabia has been honing its ability to respond rapidly and monitor and control the spread of disease — both now and in the case of any future outbreak.
The Kingdom has attributed much of its success in stemming the tide to its early adoption of digital technology to help it monitor the spread of COVID-19 and shape its response. The Riyadh Global Digital Health Summit, a two-day virtual conference organized by the Ministry of National Guard and the G20 Saudi Secretariat in collaboration with the Saudi Center for International Strategic Partnerships, was held on Aug. 11-12 and attracted more than 135,000 registered participants from 110 countries.
Speaking on the last day, the summit’s president, Dr. Bandar Al-Knawy, CEO at Health Affairs, Ministry of National Guard and president of the King Saud bin Abdul Aziz University for Health Sciences, said that the organizers had been “really overwhelmed with the level of enthusiasm across the globe,” which had made this “one of the largest virtual events ever witnessed.”
The result of the summit was the Riyadh Declaration, a manifesto for “The Role of Digital Health in Fighting Current and Future Pandemics,” forged over a series of meetings of a panel of experts from Saudi Arabia, the UK, the US, France, Australia and South Korea.
The summit also reflected the reality that, even as the battle against COVID-19 continued, scientists and governments were turning their attention to the next pandemic that many believe is inevitably heading our way.


During the pandemic the world – and world leaders – became used to doing business online. "We have a duty to rise to the challenge together during this summit and give a strong message of hope and reassurance," King Salman said during his opening speech to the virtual G20 summit in November 2020. (SPA)
During the pandemic the world – and world leaders – became used to doing business online. "We have a duty to rise to the challenge together during this summit and give a strong message of hope and reassurance," King Salman said during his opening speech to the virtual G20 summit in November 2020. (SPA)
In April 2020, scientists working with the Smithsonian’s Global Health Program discovered six new coronaviruses in bats in Myanmar. Although “none of the viruses appeared to be closely related to SARS-CoV, MERS-CoV, or SARS-CoV-2,” they reported in the journal PLOS One, it was not yet clear if the new viruses were potentially harmful to humans.
But even if they are not, the odds are high that a new coronavirus threat will emerge; bats alone are thought to harbor more than 3,000 as yet undiscovered coronaviruses.
Although the final assessment of the pandemic’s human and economic costs will be enormous, “the current crisis will eventually end,” wrote Prof. Michael Osterholm, director of the Center for Infectious Disease Research and Policy at the University of Minnesota, in Foreign Affairs in July 2020.
But he warned, “the public health community has for years known with certainty that another major pandemic was on the way, and then another one after that (and) some future microbial outbreak will be bigger and deadlier still.”
The COVID-19 pandemic, added Osterholm, “is probably not ‘the Big One,’ the prospect of which haunts the nightmares of epidemiologists and public health officials everywhere.”
Under the banner of its G20 presidency, Saudi Arabia unified the world in recognition that global collaboration is the only way forward if the world is to be better placed to fight off its next, inevitable microbial enemy.
This message was reinforced on Aug. 13, 2020, in a speech by the WHO’s director-general, marking the sixth-month anniversary of the designation of the COVID-19 outbreak as a public health emergency of international concern.
Back in January, he recalled, there had been just 100 cases outside China and no deaths. Since then, he said, “there has been an exponential rise in cases, and every country in the world has been impacted.”
By Aug. 13, the day he spoke, there had been a total of 21 million cases and over 756,000 deaths around the world.
“Everyone,” said Ghebreyesus, “is asking, ‘So how do we go back to ‘normal?’ And today, I want to talk about not how we’re going to go back, but how we’re going to go forward — and that to move forward, the best bet is to do it together.”
In the achievement of that ambition — over two extraordinary years in which Saudi Arabia’s standing on the global stage has grown immeasurably — the Kingdom has led the way.
Hear everyday Saudis talk about their lives during the COVID-19 pandemic and how they managed to find a bright side.
Credits
Writer: Jonathan Gornall
Editor: Mo Gannon/Tarek Ali Ahmad
Designer: Omar Nashashibi
Graphics: Douglas Okasaki, Farwa Rizwan
Video producer: Eugene Harnan
Video editor: Hassenin Fadhel
Video interviewer: Hussam Al-Mayman
Videographers: Mohammed Al-Baigan, Nuaf Al-Mutery, Abdullah Almdefer
Photo research: Sheila Mayo
Copy editors: Sarah Mills, Les Webb
Social media: Mohammed Qenan
Producer: Arkan Aladnani
Editor-in-Chief: Faisal J. Abbas


